Since 1991, conflict and statelessness profoundly affected the health care system in Somalia. After the collapse of the central government and the descent into civil war, many efforts to restore a central government were unsuccessful. Powerful internal forces and regional dynamics resulted in a state of chaos.
The impact of lack of governance has resulted in a generation without adequate access to social services and the collapse of public institutions for health and welfare. Despite the success of some business sectors, Somalia is marred with widespread social and economic problems and a dire lack of public social amenities. In 1991, the North West region declared an independent republic of Somaliland. Later, in 1998, the north east declared itself as autonomous state of Puntland. The south central zones of Somalia remain locked in intermittent conflict and violence.
Literature review indicates, even before the outbreak of the internal conflict, the health systems in Somalia was rather weak and underfunded. After 19 years of conflict, the health systems in Somalia remains underdeveloped poorly resourced, inequitable and unbalanced. It struggles to provide services to a limited number of Somalis against crushing constraints. Insecurity, geographical challenges and nomadic populations, unstructured and unskilled workforce, lack of motivation and division, uncertainty about the political future and administrative setting are key issues that the Somali Health system is facing.
The ministry of health’s ability to coordinate and monitor health services is almost absent. The public health care network is small. It most relies on national and international NGO’s that are concentrated in towns and secure areas. The health workforce are few, under skilled and ageing often engaged in private and public practices.Limited access due to insecurity in central and south Somalia has restricted health activities contributing the spread of diseases such as acute respiratory tract infections, obstetrical problems, anaemia, and sexually transmitted infections. In addition, injuries resulting from armedconflict are common but few health facilities have the capacity to treat them. In some areas, war-damaged hospitals and clinics have been rebuilt and qualified health professionals are returning to practices, but the overall health situation in Somalia remains worse with some of the worst health indicators in the world.
SFH Integrated health program envision to:
Increased access to essential package of health services, maternal health services and improved quality of care for the target populations.
In Lower juba, SFH:-
- Support 4 MCH and 6 health posts with staff, drugs and medical equipment’s to provide diagnosis, treatments and emergency referrals.
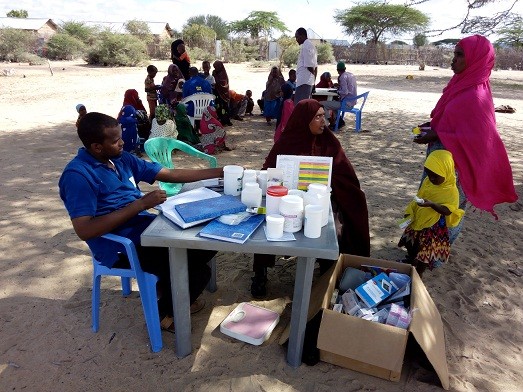
- Provides refresher trainings to all levels of health workers in our static health facilities and health post, to ensure timely and quality responses are delivered in case of outbreaks and in post recovery situations.
- Health centres provides skilled birth attendance and emergency obstetric care services.
- All health facilities provides free PNC /ANC services
In general, our health facilities record an average annual consultations, treatments and referrals of 12,000 patients